 |
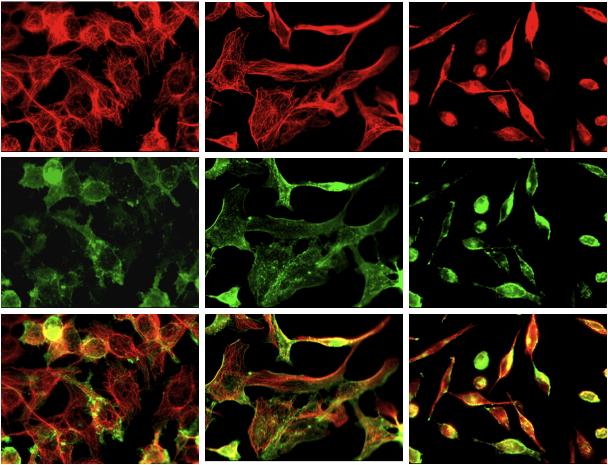
| Human breast cancer cells treated left to right with dasatinib. The same samples are dyed to highlight different proteins. Photo courtesy of Dr. Corey. |
Researchers at Northwestern University are pioneering ways to shoot out the tires from breast cancer’s getaway car in a high-speed chase of drug assassins and carcinogenic criminals.
 |
| Dr. Seth Corey, M.D. |
That’s because breast cancer itself doesn’t kill until it metastasizes, or travels, to other sensitive organs, invades and then grows. But a new clue to stopping this destructive spree surprisingly came from children.
Dr. Seth Corey is a pediatric oncologist at Children’s Memorial Hospital and professor of cellular and molecular biology at Northwestern University’s Feinberg School of Medicine. He and his researchers saw similarities between the travels of breast cancer and another notorious roamer – leukemia. They found that dasatinib, a drug already used to eliminate leukemia in the bone marrow, may also prevent mobility in breast cancer, keeping it from jumping the mammary ship to invade vital organs and kill.
But even though dasatinib is FDA-approved for the treatment of leukemia, the likelihood of your doctor prescribing it for breast cancer just yet is slim. The Northwestern research team hopes to take advantage of dasatinib’s clinical breast cancer trials to determine what responds best. By mapping the biological signatures of varying cancer types this way, fingerprints of these malignant flight-risks to assist in diagnosis and further targeted treatment may not be far off.
Corey details the research of his team and what the future may hold for dasatinib and certain kinds of breast cancer:
Corey details the research of his team and what the future may hold for dasatinib and certain kinds of breast cancer:
Q: What makes breast cancer unique among cancers?
A: I’m a pediatric oncologist and even though death due to cancer remains the most common cause of non-accidental death in children and adolescents, it’s uncommon. Maybe about 12,000 cases of new pediatric cancer are diagnosed each year in the United States. The total for adult cancers is about 1.5 million people each year, so pediatric cancer is basically one 100th the frequency of adult cancer.
Every cancer is different, and even within different [cancers] there are different types and different levels of aggressiveness. Breast cancer is a public health concern because around 180,000 women are diagnosed each year with breast cancer, so it’s one of the most common cancers to occur.
Q: What is the basic aim of your research?
A: My primary interest is in leukemia, which is a cancer of the bone marrow – the site of [all] blood cell production. Cancer cell behavior is this: they proliferate, they do not differentiate, and they do not die. But for solid tumors, which is everything but leukemia, the cancer cells also have additional characteristics that make them malignant and that is the ability for them to invade local tissues and to spread to different sites and to metastasize as in the liver, the bone, the brain. Those are the more common sites for breast cancer metastasis.
So we were primarily focused on the liquid tumors, like leukemia, but we were also interested in what were the signals intracellularly that make a cancer cell a cancer cell in addition to the signals that deregulate growth, death and maturation. We were also interested in what we call “cytoskeletal rearrangement,” or the reorganization of a cancer cell that allows it to invade and to metastasize. And that was sort of our rationale for getting more interested in breast cancer.
Q: Is leukemia a very common cancer in children?
A: Acute lymphoblastic leukemia (ALL) is the most common type of childhood cancer, although in adults it’s very rare. ALL occurs with about 3,500 cases per year, so it’s a little less than a third of all pediatric cancers.
ALL has been the focus in childhood cancer and, over the past 40 years or so, it has gone from a disease that was almost uniformly fatal to a disease that’s almost uniformly curable. We’ve gone from a roughly five year survival rate in about 1960 or so of 8 percent to a five-year survival rate in 2010 of like 90, 92 percent. It’s been an achievement of modern chemotherapy.
Q: So how did leukemia in children lead you to study breast cancer?
A: When I was a fellow in pediatric hematology studying leukemia and trying to figure out what were the growth promoting enzymes and molecules inside a cell that cause a cell to become cancerous, I identified a group of enzymes that are known as the “Src kinase” – Src (pronounced “sark”) for sarcoma.
Src kinase is an enzyme, which is a protein that speeds up chemical reactions a million-fold. It remodels the cytoskeletonand the plasma membrane [of a cell]. A cell, whether it’s normal or cancerous, has [a plasma] envelope around it. It keeps the contents in and permits information to be passaged internally. So this protein was important because it remodels the envelope of the cell as well as reorders the scaffolding of the structure of the cell. We started to look in the mid 1990’s at the first class of Src inhibitors – or drugs that will block the enzyme activity. And we had some success in test tubes showing that these will block leukemia. So, because Src also plays a role in the cytoskeletal rearrangement, we started to take a look [at it in breast cancer].
Christina Pichot gets a lot of the credit for helping to steer the lab and my thoughts in the direction of breast cancer. Chrissy was a graduate student then, she just got her PhD in March, and she was interested in breast cancer. She began to take a look at Src kinase and how its levels and expression patterns correlated with different types of breast cancer and found that levels were highest in those breast cancer tissues that were the most aggressive and invasive. What she did was manipulate the expression of this protein by turning it off. And she found that cells didn’t invade as well, didn’t migrate as well and didn’t form finger-like projections, invadapodia, which help break down the barrier and facilitate the initial steps in cancer cell invasion. When cancer cells take up residence and continue to grow forming metastasists, that’s what kills people.
Chrissy started to take a look at a drug, dasatinib, which is an FDA approved drug for a form of leukemia called Chronic Myeloid Leukemia (CML). We found that [blocking] the Src kinases didn’t so much stop the cells from surviving. It kind of got them to stop growing as quickly. But what it also did, and I think this is something that needs to be exploited, is that it did affect their ability to migrate, to invade and to form those finger-like projections of invadapodia.
Q: How can readers imagine this for themselves?
A: You can think of it like a car. A car needs to move and the way it moves is turning on the engine and running on the four tires. So the idea is to knock out all the tires so our cancer car won’t move. If you can shoot out the tires of the car with a drug like dasatinib then you’re going to slow down the cancer cell and extend peoples’ lives.
Q: How close is this to something that can be used in current treatments for breast cancer?
A: Well, dasatinib is an FDA approved drug for patients with CML as an acceptable form of treatment. It’s currently in what we call Phase I and Phase II [clinical trials for breast cancer]. Phase I is dose finding and toxicity determination studies. Phase II trials are to determine efficacy and I think that’s where the drug is.
We know from cancer therapy that a single drug is not going to work for almost all cases of cancer so there the issue is looking at combinations of drugs and that gets more difficult to do. Drug companies look for some possibility of efficacy so they can decide to continue with the drug development. What we like to do in our work is to encourage further drug trial design incorporating dasatinib into a regimen that includes other cancer drugs.
Q: Is dasatinib something someone who currently has breast cancer can ask their doctor about?
A: Well, there are frontline and second line salvage therapies. If you fail [frontline], then you go to a second line therapy. Some of that depends on the tissue type of the breast cancer. We need to define which patients will respond to dasatinib containing regimens and that’s where we want to move the field forward. We believe there is a role for dasatinib in preventing local disease from becoming metastatic but these trials have to be carefully designed.
We believe that in women with aggressive [breast cancer], dasatinib should be included in the multi-drug regimen, the question is how to introduce it. And that’s a difficult issue. Patients that have gotten all these different drugs tend to be chemo-resistant and if you give a drug like dasatinib to a woman whose breast cancer has seen a lot of drugs and have become resistant, the likelihood of seeing a positive result is very low – by itself or with other drugs. That’s a big hurdle to overcome.
Q: So is it ideally for someone who’s been recently diagnosed rather than a patient whose disease is more advanced?
A: One goal is to make the disease go away, but an alternative goal is to have stable disease in check. Status quo. I think a lot of people would like that as a goal if you can’t cure somebody of a cancer, you can make it a chronic disease. I think most people could live with that. The question is how to incorporate dasatinib into a multi-drug regimen as a second line or third line therapy for women with refractory, or relapsed, breast cancer.